Thoracic Outlet Syndrome (TOS) (Folder)
5623 EJ Eindhoven
040 - 239 91 11
Thoracic Outlet Syndrome (TOS) (Folder)
You have been referred to the TOS Expert Centre Catharina Hospital. This brochure will tell you more about TOS as a disorder, the tests you might undergo in our center as well as the treatment options we can offer.
What is thoracic outlet syndrome?
Thoracic outlet syndrome (TOS), also called shoulder girdle syndrome, is a collective term for conditions caused by entrapment of the vascular nerve bundle in the shoulder area.
Cause of Thoracic Outlet Syndrome
Thoracic outlet syndrome (TOS) is caused by anatomical structures that cause the vascular nerve bundle in the shoulder area to become pinched. The area where this impingement occurs is called the thoracic outlet. The thoracic outlet is a narrow space through which the vascular nerve bundle runs. This vascular nerve bundle consists of the subclavian artery and vein and the brachial plexus (nerve bundle). This space is bounded by the scalenus muscles/short neck muscles, the first rib and clavicle (collarbone) and the space below the pectoralis minor muscle (small pectoral muscle).
In people with TOS, when the arm is raised, this space becomes narrower, causing the vascular nerve bundle to become pinched. This is especially common in certain professions (hairdressers, painters), people who play certain sports (e.g. swimming, baseball, volleyball, handball) and people who have had a car accident or trauma (hard fall collarbone fracture) in the past.
The combination of a congenital, abnormal anatomy and a past trauma can be indicated as the cause of TOS in approximately half of the TOS patients.
The anatomy – information about possible entrapment
The three anatomical spaces where impingement may occur are the scalene triangle, the costoclavicular space and the pectoralis minor space (see Figure 1)
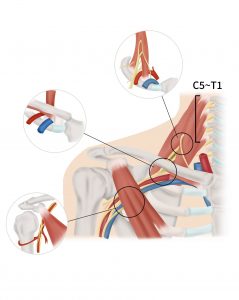
Figure 1: Where does it pinch? Scalenus triangle, Costoclavicular space and/or Pectoralis minor space
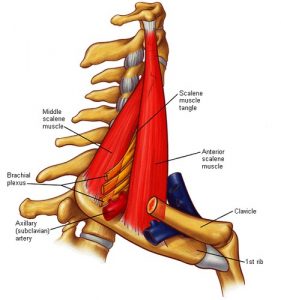
Figure 2: The scalenus triangle Source: Edoctoronline.com, www.edoctoronline.com, March 16, 2017
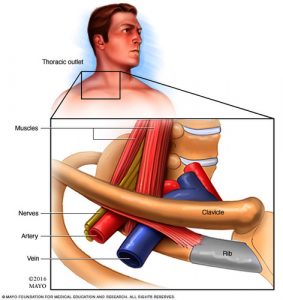
Figure 3: The costoclavicular space Source: Mayo Clinic, www.mayoclinic.org, March 16, 2017
Scalenus triangle
The scalenus triangle is the most proximal site of entrapment in the thoracic outlet region. The scalenus triangle is located above the first rib where the brachial plexus (nerve) and subclavian artery together pass between the middle and anterior scalenus muscle (short neck muscle) (see Figure 2). Impingement in the scalenus triangle is often associated with head and neck pain. These two muscles assist in turning the head and can help with breathing.
The costoclavicular space
The costoclavicular space is a potential site of impingement located below the clavicle (clavicle) and above the first rib (costa). Between the clavicle and the first rib, the brachial plexus continues its path to the arm. In addition to the brachial plexus, the subclavian artery and vein also run through this anatomical space (see Figure 3). Hence, an impingement of the vein or artery can occur here in addition to an impingement of the nerve. On the first rib or on a so-called cervical rib (see below) ligaments (bands) can attach themselves which can run tightly along the nerve, vein or artery and thus contribute to the compression of these structures.
Pectoralis minor space
The pectoralis minor space is the most distal compression site and is named after the muscle under which the vascular nerve bundle travels: the pectoralis minor (small chest muscle) (see Figure 1). Underneath this muscle, the nerve, vein and artery run into the arm. A thickened muscle or scarring can cause these structures to become pinched under the muscle.
Cervical ribs
Cervical ribs are congenital bony structures not found in the “normal” anatomy of the neck. These cervical ribs can provide an additional compression site and therefore may play a role in the development of Thoracic Outlet Syndrome.
Intake
The intake is the first meeting you have with our TOS team. Based on your symptoms and the referral from the general practitioner or medical specialist at another hospital, an appointment is made with the vascular surgeon and nurse specialist, and/or the neurologist and/or the orthopedic surgeon and/or the physiotherapist.
During this meeting, your symptoms will be assessed and a physical examination will be performed. In consultation with the TOS specialist, any additional examination will be initiated after the intake. Beforehand a questionnaire will be sent to you. With this questionnaire an increase or decrease of the complaints will be measured during the time that you are being treated or followed in our center.
Different subtypes of TOS
There are three subtypes of TOS:
*A neurogenic variant (NTOS).
*A venous variant (VTOS).
*Arterial (arterial) type (ATOS).
The literature shows that in 95% of cases, the primary cause is neurogenic (NTOS), in 4% venous (VTOS) and in 1% arterial (ATOS). Combinations of these three subtypes are possible and frequently encountered. This patient information brochure describes all 3 subtypes.
Neurogenic Thoracic Outlet Syndrome (NTOS)
How do we make the diagnosis NTOS in the Catharina TOS expert centre?
The diagnosis of NTOS is based on four pillars:
*Your symptoms and history;
*The findings on physical and additional examinations;
*The absence of any other explanation for the symptoms;
*The result of a trial blockade (an injection into the cervical or small pectoral muscle).
Complaints and history
The majority of patients with thoracic outlet syndrome (TOS) present with complaints related to the brachial plexus. This affects approximately 95% of all patients, most common in females (4:1 ratio) between 20 and 40 years of age. The complaints of this entrapment can largely be divided into groups, namely, pain and numbness of the arm, pain in the chest wall, shoulder, armpit, neck, back of the head and / or back pain. In addition, there may be a tingling sensation, loss of strength and/or a numb or fatigued feeling in the arm and/or fingers.
The findings on physical examination
The physical examination will attempt to elicit the symptoms you are experiencing. Some provocation tests are used (provocation = elicitation).
At the Catharina TOS Expert Centre we use the Upper Limb Tension Test (ULTT), in which the symptoms are provoked by raising the arm and tilting the head away. In addition, the Elevated Arm Stress Test is used, in which the arms are raised to an angle of 90 degrees and the hands must be opened and closed for 3 minutes. In our center we developed a standardized EAST meter to obtain uniform test circumstances. We also check for nerve irritation by applying light taps to the skin at a few places. With pressure at places where the nerve can be pinched (irritated), it is observed whether the symptoms occur and/or increase.
A positive result from one or more of these tests is no guarantee of having NTOS, it only gives direction to the diagnostic process.
Additional examinations
In addition to the physical examination, we use several additional tests:
Research in our center revealed that Duplex examination is not discriminating between patients with and without NTOS and thus of no value in the diagnosis of NTOS.
X-ray of the upper part of the chest is taken to detect any abnormalities of the clavicle, first rib and/or any cervical rib(s) as well as a regular chest X-ray.
CT examination: in case of abnormalities of the rib, a cervical rib, or other abnormalities of the bones in the shoulder girdle area, to better understand the anatomy, a 3D-CT scan is sometimes performed.
Electromyogram: In some cases, the Neurologist will order an electromyogram (EMG). This is a muscle and nerve examination that records the electrical activity of various muscles and nerves. It is NOT conclusive for NTOS, though can be used to see if the nerves have suffered (permanent) damage due to other causes than NTOS
The absence of another explanation for your symptoms
The various specialists in our TOS team will, on the basis of their own expertise, examine whether other causes may underlie your symptoms. This also happens if you have been to other specialists before. Among other things, they will look at possible limitations in movement of the neck, muscle disorders, disorders of and around the shoulder joint, disorders of and around the elbow joint, pinching of the nerve at the level of the elbow and disorders in and around the wrist.
Physiotherapeutic assessment
When nerves in the so-called thoracic outlet become pinched during specific postures or movements, a physiotherapeutic course with postural correction can sometimes offer a solution. The physiotherapist you visit at our center is an external physiotherapist who is present within the TOS Expert Centre for your convenience. As a result, this visit is cannot be covered by hospital-insured care and will be charged directly to you
The physiotherapist who examined you will indicate to what extent the course of physiotherapy (if any) you have already undergone was adequate. If the physiotherapist indicates that he or she sees possibilities for improvement through physiotherapy, a course of physiotherapy will be started first. This can be done in your home environment. The physiotherapist connected to our TOS team will contact a physiotherapist in your living community who is demonstrably experienced and will discuss an exercise schedule.
The Trial Blockade
The trial blockade is used as part of the diagnosis when a NTOS is suspected. The placement of a trial blockade is done in the Department of Pain Medicine. During this examination, it is investigated whether the muscles in the neck are clamping the interstitial nerves. A small amount of anesthetic is injected resulting in the temporary relaxation of these muscles. This gives the nerves more space and if the cause is the entrapment of the muscles, symptom reduction occurs.
You will be asked by the specialist to lie on your back so that the neck is easily accessible. Under ultrasound guidance, a needle is placed very precisely twice and a small amount of anesthetic fluid is injected into both muscles. Then the needle is removed and the procedure is over. The entire procedure takes about 30 minutes.
Because of the use of ultrasound equipment, the technique is safe and the specialist can properly locate the muscles. Therefore, the risk of complications, such as nerve or vascular damage, during this procedure is very low.
Results
Before and 30-60 minutes after the test blockade, the standardized EAST will be performed. You will also be given a 3 day diary and asked if, and if so on what scale, your symptoms have decreased. These results will be compared to the measurements taken prior to the test blockade. You will then be given a score list (diary) to take home with you on which you can indicate how you experienced the symptoms during the day of the test blockade and the following days. The nurse specialist will discuss these results in the multidisciplinary consultation with the other TOS specialists.
Side effects
After the treatment you may experience temporary loss of strength in your arm. This loss of strength is due to the use and overflow of the anesthetic fluid to the nerves. In doing so, temporary numbing of other nerves in the neck may also occur, causing a temporary hoarseness or drooping of the eyelid. In very rare cases, you may experience some shortness of breath for a short time. The above side effects last for a few hours and then subside. If you have any questions about side effects for a longer period, please contact the outpatient clinic of Anesthesiology and Pain Medicine at 040 – 239 85 00.
Important information for your appointment
Please inform the Department of Anesthesiology and Pain Medicine before treatment if you are (potentially) pregnant.
After the treatment, you may not actively participate in traffic on the same day. Hence you will have to arrange your own transport home.
Anticoagulants (blood thinners) that require monitoring by the thrombosis service must be stopped, depending on the drug, two to seven days before the treatment. This is done in consultation with your doctor. Prior to the treatment, your blood (INR value) will be checked. If these blood clotting values are not in order, we will postpone the treatment to another date. In consultation with the anticoagulation clinic, you will start taking your anticoagulants again in the evening.
If you are taking other anticoagulants, such as an antiplatelet agent (acetylsalicylic acid, ASA, Ascal, Clopidogrel, Grepid), or a DOAC (Pradaxa, Xarelto, Eliquis,etc.), you should discuss with your doctor how long this should be discontinued before the trial blockade.
If you are allergic to certain medications you should disclose this before treatment.
Diagnosis
In order to obtain a complete picture of your symptoms, the questioning of your symptoms and the physical examination will be carried out by a vascular / TOS-surgeon, neurologist, nurse specialist or physician assistant and physiotherapist. In some cases you will also be examined by the orthopaedic (shoulder-) surgeon of our TOS-team. your case will always be discussed in a multidisciplinary consultation (MDO). In this meeting all examinations are discussed and advice is given for further treatment.
Surgical treatment of NTOS: Thoracic Outlet Decompression (TOD)
When are you eligible for surgery?
If all four pillars point to NTOS and the physiotherapist of our TOS team indicates that there is no room for improvement by non-surgical means, you will be discussed again in our multidisciplinary consultation. All complaints, examinations and results will be discussed again. Based on this information, the decision is made whether you are eligible for surgery: a so-called Thoracic Outlet Decompression (TOD). In this procedure, the lower part of the brachial plexus is exposed and completely freed (neurolysis). On indication, the small pectoral muscle (pectoralis minor muscle) will be partially resected. The vascular surgeon will discuss the procedure and the pros and cons of the operation with you in a meeting at the TOS outpatient clinic. Clarifying explanations regarding a Thoracic Outlet Decompression can be found further on.
Venous Thoracic Outlet Syndrome (VTOS)
What is a Venous Thoracic Outlet Syndrome (VTOS)
Venous TOS (VTOS) is the venous variant of TOS. This means that the vein has become trapped and/or repetitively damaged.
Symptoms with VTOS
Common symptoms of VTOS are swelling of the arm, discoloration of the arm and/or visible veins in the arm, shoulder, breast. These symptoms can increase when lifting or using the arm. The symptoms can also subside when holding the arm still. If the above symptoms have arisen suddenly, do not subside even when the arm is at rest and is painful, this is a reason to consult a doctor urgently. It is possible that this is an upper extremity deep vein thrombosis (UEDVT).
Patients with an UEDVT are seen at the TOS outpatient clinic or in the emergency department (preferably as soon as possible but no longer than 10 working days after the onset of symptoms). Please note that in the event of an UEDVT, blood thinners must ALWAYS be started as first line treatment (this can be done through your own GP/local hospital).
Consequences of a venous thoracic outlet syndrome (VTOS)
As a result of a VTOS, an arm vein thrombosis (UEDVT) may occur. This is also known as the Paget-Schroetter syndrome or effort trombosis. An arm vein thrombosis is an occlusion of the arm vein by a blood clot and is an urgent indication to consult a (general) practitioner.
How is the diagnosis of VTOS established?
The diagnosis of VTOS, UEDVT or post-thrombotic syndrome (complaints after an UEDVT) of the arm can be made on the basis of a number of investigations:
Duplex (ultrasound) examination of the arm vessels: A duplex examination is designed to detect any abnormalities in the veins. This examination looks at the blood flow in the veins. The examination is performed by a laboratory technician from the vascular laboratory. During this examination, various (provocative) positions are adopted.
X-ray of the upper part of the chest is taken to detect any abnormalities of the clavicle, first rib and/or any cervical rib(s) as well as a regular chest X-ray.
Phlebography: This examination is used to visualize the veins in the arm and at the level of the shoulder girdle. This helps to determine how the veins run and whether they are narrowed or occluded. Contrast medium is injected into a blood vessel on the arm or hand via an infusion needle, after which a series of x-ray photographs of the blood vessels filled with contrast is taken. For these pictures, the arm is placed in different positions to visualize any narrowing. The examination lasts approximately 30 minutes.
Treatment of VTOS
Thrombolysis
In the acute form of VTOS, in which an arm vein thrombosis has occurred (Paget-Schroetter syndrome), patients benefit from rapid thrombolysis (dissolving the clot with drugs). This thrombolysis is performed during hospitalization.
Surgical intervention in VTOS
Following successful thrombolysis in case of acute thrombosis, decompression of the thoracic outlet is performed. The vein is also completely exposed and freed from compressing surrounding elements (venolysis). Subsequently, in the same session as your operation, a phlebography is performed on the operating table and an assessment made as to whether (almost always the case) the vein needs to be dilated (stretching of the vein with a high pressure balloon: angioplasty procedure). Clarifying information about this procedure can be found further on.
In patients with VTOS without thrombosis (McCleery’s syndrome or post-thrombotic/chronic VTOS), there is no indication for thrombolysis and decompression of the thoracic outlet is only necessary if the severity of the symptoms in relation to work/sport justify this. Extensive venolysis and a angioplasty procedure are also performed in these cases. This will be discussed in detail with you at the outpatient clinic of our TOS center
Arterial Thoracic Outlet Syndrome (ATOS)
What is an Arterial Thoracic Outlet Syndrome (ATOS)?
Arterial Thoracic Outlet Syndrome (ATOS) is the arterial variant of TOS. In this case, the artery in the thoracic outlet has become trapped and damaged. Compression of the artery without further sequelae is not ATOS.
Symptoms in ATOS
Complaints that are common with ATOS are:
*A tired and heavy feeling in the arm; especially when using the arm.
*A cold feeling in the arm, pale or mottled fingers and/or muscle cramps.
*Discoloration of the fingertips.
*Pain in the arm and/or hand.
Also in this form, the symptoms may arise or increase when lifting or using the arm. Such a pattern of complaints in a young, fit patient has few other causes. Nevertheless, this form of TOS also requires additional examination to determine the exact location of the entrapment and whether vascular damage has occurred.
How is the diagnosis of ATOS established?
The diagnosis of ATOS can be made based on a number of examinations:
X-ray of the upper part of the chest is taken to detect any abnormalities of the clavicle, first rib and/or any cervical rib(s) as well as a regular chest X-ray.
CTA examination: In addition, a CT scan of the arteries in the arm and shoulder is often performed. In this examination, contrast medium is injected into the bloodstream and then a CT scan is made. Because the contrast in the bloodstream can be clearly seen on the scan, the course of the arteries can be viewed.
Consequences of an Arterial Thoracic Outlet Syndrome
As a result of repetitive constriction, damage to the artery wall can occur, causing thromboembolisms (blood clots) that can cause acute symptoms. These embolisms end up in the fingers/thumb and close off the artery, which can lead to necrosis of (part of) the finger(s). The subclavian artery can also become aneurysmal (dilate) due to prolonged entrapment.
Treatment of ATOS
Surgical treatment of ATOS
When treating ATOS with the appearance of thromboembolisms, conservative therapy (exercise, different lifestyle, etc.) is often not an option. This means that the treatment of ATOS consists of surgical intervention. In this surgery, the entrapment is remedied by decompression of the thoracic outlet, correcting any source of thromboembolisms (blood clots). In the process, you will receive medication (platelet aggregation inhibitors) to reduce the risk of blood clots and/or clot formation. Clarifying information about the procedure can further on.
Thoracic Outlet Decompression
Care prior to surgery
The anesthesia department conducts a preoperative screening. Your overall health and expected risks during surgery are assessed. If possible, especially for patients from outside The Netherlands, this screening will take place after your last appointment at the TOS outpatient clinic.
Three or two days before surgery you will receive a call from the admissions department with information about your admission. You will be told, among other things, which medications you may still take, whether you must be sober (no eating, drinking or smoking before surgery) and where in the hospital you may report. Depending on the time of surgery, you will be admitted to the hospital either the day before or the day of surgery.
Procedure during surgery – Thoracic Outlet Decompression (TOD) surgery
Surgery may be performed through the armpit (transaxillary approach) or through an incision above the collarbone (supraclavicular approach). Sometimes an incision is made both above and below the collarbone (paraclavicular approach). The incision through the armpit is preferred in our center because of better cosmetics on one hand and the possibility of performing a second operation above the collarbone if symptoms return. Removing a cervical rib and/or transecting the small pectoral muscle can all be done through this axillary (transaxillary) approach.
TOD surgery always consists of removing the entire first rib (so called ‘cartilage to cartilage’ first rib resection), including partial removal of the short cervical muscles attached to the rib and any fibrous bands that are trapping the vascular/nerve bundle (see Figure 4 and 5). “Neurolysis” (freeing the nerve from “fibrotic” tissue), “venolysis” (freeing the vein from “fibrotic” tissue) and/or arteriolysis (freeing the artery from “fibrotic” tissue) is performed as part of TOD surgery. Going through the muscles and ligaments (bands) will not affect your range of motion after surgery
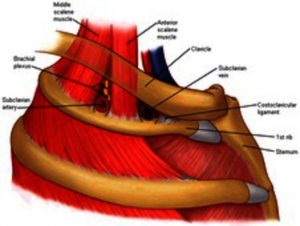
Figure 4 shows the situation before surgery (source: Institute for Neuropathic Pain www.neuropathie.nu; March 16, 2017).
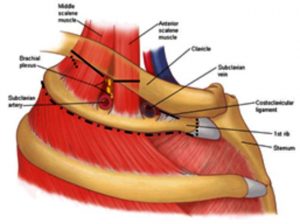
Figure 5: Situation after surgery. The black (dotted) line indicates which structures are passed through to create space (source: Institute for Neuropathic Pain, www.neuropathie.nu; edited by Prof. Dr. J.A.W. Teijink; Vascular Surgeon Catharina Hospital).
Additional angioplasty procedure after thoracic outlet decompression with VTOS
If there is a venous problem, the procedure is combined with an angioplasty procedure because almost always scar tissue has also formed on the inside of the vein, caused by chronic irritation. During a angioplasty procedure, a balloon in the blood vessel is inflated under high pressure to reopen or dilate the blood vessel. During surgery, it is checked to see if blood flow through the vein has been restored. Exceptionally, a stent may be placed to keep the vein open properly. No long-term results are known (yet) about the placement of a stent in this situation, which is why we are very reluctant to do so.
Additional treatment after thoracic outlet decompression with ATOS
In thoracic outlet decompression, the entrapment of the artery is relieved. In the process, any source of thromboembolism (blood clots) may be corrected (for example, with a bypass). In these cases, a supra- or paraclavicular approach (incision above or above and below the clavicle) is chosen. Sometimes there is dilation of the artery behind the entrapment (a so-called post-stenotic dilatation). After TOD, in which the entrapment is removed, it is not always necessary to replace the dilated artery. However, after surgery you will continue to be monitored and this dilatation will be checked in time for any growth.
Risks of surgery
Complications may occur with any surgery. With this surgery, there is a risk of the following complications:
Neuropathic (pain) complaints (complaints caused by irritation / damage to a nerve): numbness, pain or an unpleasant, sometimes burning / painful sensation on the inside / dorsal side of the (upper) arm. This occurs because during the operation a small nerve, the nervus intercosto-brachialis II, must be kept aside where it can be stretched. Often these symptoms subside after 6 to 12 weeks. In exceptional cases, this nerve even has to be transected in order to perform the operation safely and properly.
In a portion of patients, a defect in the lung membrane arises as a result of the sliding of the lung membrane against the rib. This is not a collapsed lung as is sometimes claimed and in most cases has no consequences for your treatment (length of stay in hospital) and can in most cases be resolved via the standard wound drain (a tube from the wound). In some cases an additional X-ray is taken the morning after the operation. Sometimes a cut is deliberately made in the lung membrane during surgery to allow excess wound fluid/blood to drain from the operated region. Through a special tube in the chest cavity, this is sucked out again. The risk of a pneumothorax, for which a drain must be placed AFTER surgery, has not occurred in the last 150 patients.
Post-operative bleeding: Especially in procedures where anticoagulants are started shortly after surgery, there is a risk of post-operative bleeding. Usually bleeding stops by itself and the blood is drained through the tube (or tubes: wound drain and chest drain) left behind at the surgery. Very rarely, the wound must be reopened (<1%).
Vascular damage: A vein and an artery run through the surgical area, which can be damaged during surgery. This complication occurs in 1 to 2% of surgeries performed, according to the literature. This damage is repaired during surgery. To date (April 2022)), this has not occurred in our center.
Damage of the nerve (brachial plexus): Contrary to what you sometimes find on the Internet (“a quarter of cases”), this complication is extremely rare, even 0% in publications of renowned TOS centers and fortunately also 0% to date (April 2022) in our center. Nevertheless, there always remains a small chance that damage to this nerve structure occurs during surgery, resulting in permanent nerve loss of part of the arm/hand function. Traction damage due to positioning of the arm during surgery is also extremely rare, if it happens it is most often neuropraxia and subsides in time.
Thromboembolic events: As a result of irritation of the surgical environment, there is a small risk of blockage of the blood vessel or of a blood clot being dislodged, which may cause problems elsewhere in the body.
Wound infection (<2.5%).
Post-operative care
After the operation, a chest X-ray is taken to determine whether the diaphragm is functioning well, to establish that the first rib (and possibly cervical rib) have been completely removed, and that there is no fluid and/or air between the lung membranes. A drain will be inserted during the procedure and the nursing department will monitor the drain production (amount of fluid). If the drain production is minimal, the drain will be removed the morning after the operation..
The pain experienced after surgery varies greatly between patients. After surgery you can use paracetamol and a NSAID. Of course you may indicate if this pain relief is not sufficient. After surgery you will be able to walk or move around a bit, at first under supervision. The day after surgery the physical therapist will visit you and explain which stretching exercises you can do for your neck and shoulder, teach you breathing exercises and also give you exercises to prevent shoulder problems. It is important to continue the physical therapy at home. The physical therapist at our TOS center will give you a handout. It is important to rest the arm as much as possible for 6 weeks, so physiotherapy is aimed at preventing stiffness of the shoulder joint. If you have been operated on for an arterial or venous TOS, you will also be prescribed anticoagulant medication for (at least) 6 weeks.
After surgery you will spend at least 1 night in our hospital. Depending on your pain level, we will decide, in consultation with you, whether you can go home. In the majority of cases you may and can go home the day after surgery. Approximately 95% of the TOS operated patients go home the morning after the day of surgery.
You will be advised to wear a sling for three weeks. This will give your arm sufficient rest and will also alert those around you (small children, partner) to the fact that your arm needs rest. We also advise you to put as little strain on the arm as possible for 6 weeks (no lifting, no driving, no strength training or repetitive movements).Use of the arm can be discussed at the first control appointment with the TOS-surgeon at the TOS outpatient clinic.
Pain around the incision, as well as in the neck, chest, shoulder, and scapula region may persist for 4 to 8 weeks. Reduced range of motion of the arm may be present for up to 3-4 weeks. Symptoms that existed before surgery sometimes improve immediately after surgery, but usually not until 6 to 8 weeks. The timing of return to work varies from person to person and cannot be predicted in advance. Return to work will be discussed at the first outpatient clinic visit after surgery.
After approximately 6 weeks, you will come for your first check-up with the TOS-surgeon. Three months and one year after the operation you will come for a check-up with the neurologist (in most cases this is done by telephone consultation). After this, we will contact you annually to assess you are doing (up to 5 years after surgery). Prior to each check-up, you will be sent questionnaires (or a link) to record your condition (and our results) for scientific research purposes.
TOS Expert Centre
For all forms of TOS, a multidisciplinary team works at the TOS Expert Centre of the Catharina Hospital. In recent years, this TOS expert centre has provided satisfactory help to many people, some of whom have had symptoms for years. Our patients come from all over the Netherlands and even from abroad. For this reason, a care path has been developed in which as many examinations as possible, if necessary, take place on one day. These appointments are scheduled for you by the outpatient clinic.
Nurse Specialist for Thoracic Outlet Syndrome
Nurse specialists with specific knowledge and training in the field of TOS work within the TOS Expert Centre. The nurse specialists have master’s degrees. This makes them both capable of combining nursing and medical care. The coordination of the care path, the preparation of your visit to the TOS outpatient clinic, the first intake of patients and the answering of questions (by telephone or e-mail) is done by the nurse specialist or physician assistant, of course in close consultation and where necessary with the advice of one of the TOS specialists.
The TOS team at Catharina Hospital
The TOS team at Catharina Hospital consists of two vascular surgeons, two neurologists, one orthopedic surgeon with specific shoulder expertise, four anesthetists-pain specialists, four radiologists, two nurse specialists and three physiotherapists with specific expertise in the field of TOS. In this team, we work together to rule out other causes for your symptoms in order to make the diagnosis of TOS as reliable as possible.
All patients seen by us are discussed in a multidisciplinary consultation (MDO) in which all specialties of the TOS team are present. In this consensus meeting, the specialists together make a proposal for further diagnostics or treatment. In consultation with you, the patient, a decision is then made about the course of action.
Research into TOS
At the TOS Expert Centre scientific research is carried out to improve the diagnosis and treatment of Thoracic Outlet Syndrome. To use your (anonymous) data for research, we ask for your permission at the beginning of your care path in our TOS Expert Centre.
For example, the following studies are/were performed:
The electromyogram (EMG) study: A study of the added value of the EMG, in combination with the test blockade, in the diagnostic care pathway of a neurogenic Thoracic Outlet Syndrome. Because of the initial results from this study, an electromyogram is not always performed in the current care pathway.
Brachial plexus ultrasound: The diagnostic value of imaging the brachial plexus with high resolution ultrasound (ultrasound) was investigated. This study showed that ultrasound does not have standard added value. For this reason, the TOS Expertise Centre at Catharina Hospital will only use this additional diagnostic method in certain cases.
EAST measurement: The TOS Expertise Centre has developed an EAST measurement in collaboration with the Fontys University of Applied Sciences in Eindhoven. In this study we investigate whether more information can be obtained from the EAST measurement that contributes to the diagnosis and treatment of NTOS.
The effect of surgery in NTOS (STOP-NTOS trial): Currently the effect of surgical treatment for NTOS is being compared to conservative treatment (physiotherapy).
Frequently Asked Questions
How long does the entire procedure take?
This depends entirely on the number of specialists you visit within your specific TOS care pathway the necessary examinations that are agreed upon with you.
When will I receive the results of the multidisciplinary consultation?
Within our TOS Expert Centre we work with multidisciplinary consultation. During your care path, a nurse or medical specialist will inform you that your case will be discussed in this meeting. You will only be discussed if all the tests are known. This means that when you start physical therapy you will only be discussed after this process. This is also the case if, for example, if you are waiting for a test blockade, the performance of a phlebography/CT scan, etc. The nurse specialist will call you in the week following the MDO if your case was presented and discussed.
I am on the waiting list for a thoracic outlet decompression how long will it take before I am called?
On the day you are enrolled, you can ask for an estimate of the waiting time. On average and prolonged due to COVID-19 pandemic this is 6-8 months (situation April 2022). However, this is only an indication. Due to other (urgent) vascular surgical procedures, the waiting time may be longer. If possible, you can schedule a suitable date in the future with your TOS-surgeon or the OR planning department. A few weeks before the operation you will receive a letter with an extended date. You will be called by our admissions department two or three working days before the procedure.
How long will I be hospitalized?
The average hospital stay is 1,3 days (some patients are admitted the day before surgery). Usually you can go home the day after surgery. Depending on your recovery and your well-being, admission may be prolonged.
Do you offer the possibility for my partner to stay overnight in the hospital?
No, unfortunately we do not have the possibility to do so. Below are some suggestions for an overnight stay based on TOS-patient relatives experiences:
- Onderwijshotel De Rooi Pannen Eindhoven; Kaakstraat 1, 5623 AD Eindhoven (1.5 km to the Catharina Hospital). Telephone number: +31 405001280
- B&B Hof; Gagelstraat 89, Strijp, 5616 RP Eindhoven (4.2 km to Catharina Hospital). Telephone number: +31 646117741
- Parkhotel Auberge Vincent, Park 69, 5671 GC Nuenen (6.4 km to Catharina Ziekenhuis). Telephone number: +31 402906390
How soon can I return to work after the operation?
We strongly advise you to limit your activities with the arm for 3 months. Avoid heavy lifting, heavy household chores, repetitive movements and working above your head as much as possible for three months. In addition, you should also keep car driving to a strict minimum, especially if your right arm has been operated on and you drive a manually operated clutch. During the first three weeks you are advised to wear a sling to give the arm as much rest as possible.
What painkillers can I use after surgery?
The basis consists of paracetamol, in addition we recommend to use an NSAID for 2 weeks. This will be discussed with you during the discharge interview at the department. If this is not sufficient, please contact the outpatient surgery clinic on telephone number 040 – 239 7150.
After the operation, I have more pain at the dorsal side of my upper arm. Is this normal?
When you undergo surgery via the armpit, several structures are passed, including one of the nerves that runs from the chest cavity (n. ICB2) to the arm. You may experience numbness, burning, (nerve) pain after the procedure. This will last for some time and fade away with time. If you find the pain unbearable, please contact the outpatient surgery clinic.
When do I notice improvement?
Pain around the incision, as well as in the neck, chest, shoulder and scapula region can last for 4 to 8 weeks. Symptoms that existed before surgery sometimes improve immediately after surgery, but usually not before 6 to 8 weeks.
When are the sutures removed?
The wound is closed intracutaneously (in the skin) with clear sutures. This suture will dissolve by itself. If non-dissolvable (blue) sutures were placed anyway, an appointment will be made to remove them.
When can I shower/bath?
Showering is allowed after 24 hours, bathing is not allowed for 2 weeks. Not too hot (less than 38 degrees) to prevent softening of the wound.
General Information
Questions
After reading this brochure, do you have any questions about the origin, diagnosis and/or treatment of TOS? Please send an e-mail to TOSexpert@catharinaziekenhuis.nl or contact the outpatient clinic Surgery by telephone.
Contact details
Catharina Hospital
+3140 – 239 91 11
www.catharinaziekenhuis.nl
Outpatient Clinic Surgery
+3140 – 239 71 50
Department of Anesthesiology & Pain Medicine
+3140 – 239 85 00
Radiology department
+3140 – 239 85 65